AI for healthcare, grounded in your own clinical notes and protocols.
AI for healthcare is grounded, auditable software that RMAI builds on your own clinical notes, payer rules, and patient correspondence — so visit notes, prior-authorisation packets, message triage, and referral intake are drafted, sorted, and cited in minutes, with a clinician signing off every record.
What actually slows a healthcare practice down.
The biggest constraints in a mid-sized practice are not clinical — they are operational: documentation that spills into the evening, prior authorisation, an overflowing patient inbox, and referrals that vanish between systems. Each one is a documents-and-data problem carrying real compliance weight, which is exactly where grounded AI pays back.
Clinicians spend a third of the day being clerks
Documentation, inbox, coding queries and prior-auth forms eat roughly a third of the working day, then spill into after-hours 'pyjama time'. The bottleneck is not clinical judgement — it is the senior clinician's attention, lost to typing and re-keying.
Prior authorisation is a clinical bottleneck, not just admin
Practices spend about 13 hours per physician per week on prior authorisations, and 95% of physicians say the process delays patient care. Each request is a repeated, rules-shaped chase across payer portals, phone and fax — exactly the work that steals billable clinical time.
The patient inbox has become a shadow clinic
Portal and secure-message volume keeps climbing — primary-care inbox time rose about 24% over three years (2019–2023) — and most of it lands on clinicians directly. Without triage logic, urgent messages queue behind routine ones and response times slip.
Referrals fall into black holes between organisations
Around 14% of referrals are delayed, lost, rejected or never processed, and only 7% of people who hit a referral problem were satisfied. Fax, email and PDF intake with no closed-loop tracking means patients chase updates while staff manually re-key every handoff.
What changes once the work is grounded in your own records.
Practices working with RMAI recover clinical hours and tighten the audit trail at the same time. The outcomes below are illustrative of shipped patterns; every one keeps a clinician on the final call — nothing writes to the record or reaches a patient on its own.
The questions leaders ask first.
The questions below are the ones RMAI hears in the first call — on safety, staffing, compliance, cost, and feasibility.
What the time recovered is worth.
Move the sliders for your own volumes; the benchmark shows where shipped builds have landed.
| Task | Before | After |
|---|---|---|
| Visit note (draft + sign-off) | ~2 hrs after hours | minutes in the room |
| Prior-authorisation packet | ~30 min each | < 5 min (review) |
| Urgent message, time to first-read | ~22 hrs | ~5 hrs |
| Referral intake processing | manual re-keying | same-day, tracked |
What RMAI has built for this sector.
The applications below are grounded, human-in-the-loop tools for this sector — some already built and shipped, some scoped from real briefs. Ask us which is which.
Prior-Auth Compiler
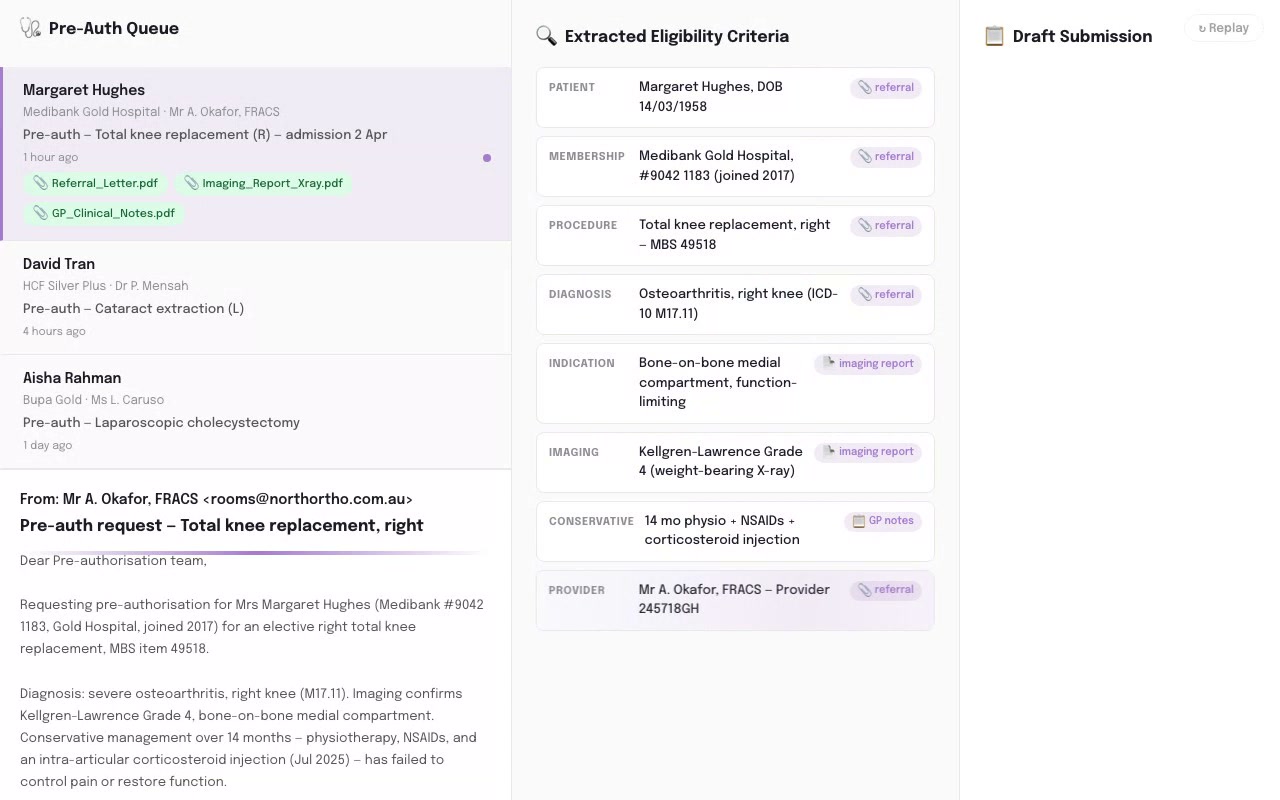
Maps the chart against payer criteria, drafts the prior-auth packet with an inline citation on every match, and flags the gaps — clinician approves before submission.
Plan Reassessment Drafter

Turns a participant's file into a first-draft plan reassessment report your coordinator edits down, instead of starting from a blank page.
No-Show Predictor

Scores each upcoming appointment for no-show risk from attendance history, SMS response and visit gaps, and flags the high-risk slots with the factors behind each — so the recall officer decides who to call before the slot is lost.
MBS Coding Assistant

Maps the services in a clinical note to the right Medicare Benefits Schedule item numbers, showing the criteria it matched and any co-claiming restrictions, so the coder checks each suggestion against the note before it is billed.
Patient-Message Triage Copilot

Sorts the patient inbox before it reaches a clinician — classifies each portal or email message, scores urgency, routes it to the right queue, and drafts a holding reply for staff to approve, while escalating anything that reads clinically urgent instead of answering it.
Denial Appeal Drafter
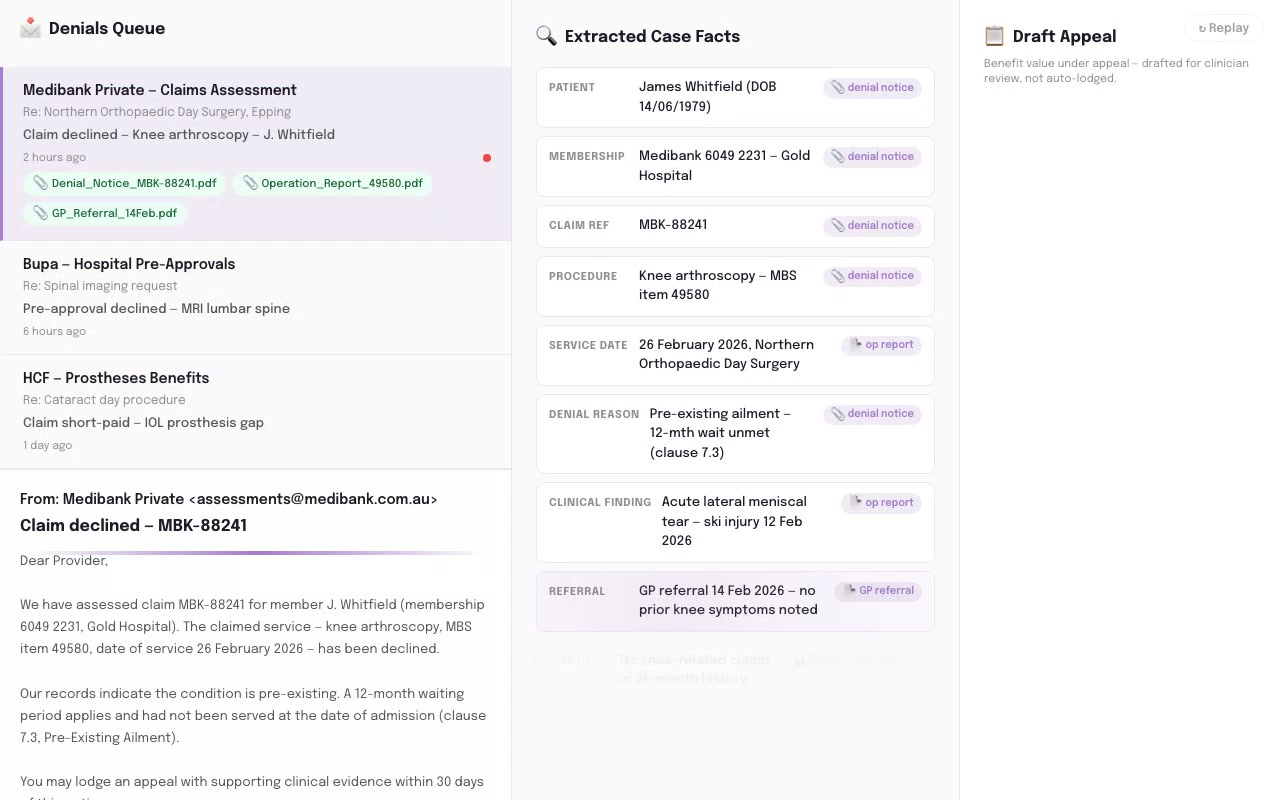
Reads the denial reason code and the chart, drafts an evidence-based appeal letter citing the relevant payer rule, and lists the documentation gaps that weaken the case.
Clinical Note Generator

Turn the consultation you just had into a structured SOAP note before the next patient walks in — drafted from the audio, reviewed and signed off by the clinician.
Complaint Response Agent

Triages every patient complaint the moment it lands, flags the clinical-safety ones, and drafts a policy-grounded acknowledgement for staff to approve.
Clinic Policy Concierge

Staff ask about an SOP, a payer rule, a consent requirement or a care protocol and get a short answer that quotes the exact section it came from — and says "not in your documents" instead of guessing.
Shift Handover Summariser

Turns a shift's scattered progress and incident notes into a one-page ISBAR-structured handover — vitals, meds, intake, mobility, falls, mood — with the source note quoted on every line and clinical risks flagged for the RN.
Reportable-Incident Signal Triage

Reads the daily progress-note flow, quotes the plain-language wording that looks like a possible reportable incident, rates its confidence, and routes it to your Approver against the 24-hour clock — flagging, never lodging.
Care Policy Concierge

Answer staff "what does our policy say?" questions from your approved document library — with the clause cited, and a refusal when the answer isn't there.
Care Policy AskMe

Answers a carer's policy or procedure question at the point of care from your own approved library — quoting the section, naming the document and version, and saying so when the answer isn't there.
Booking & Phone Agent

Answers calls 24/7, takes and confirms bookings from your own availability and menu information, sends reminders to cut no-shows, and routes anything complex or sensitive to a person with the call context attached. It works from your approved information and escalates rather than guessing.
Prompts you can use today, for free.
Sector-specific prompts RMAI uses as starting points. Copy one and run it against de-identified samples — or inside an approved private environment — to see the shape of the answer before you talk to us.
How RMAI would work with you.
Every engagement starts with the diagnostic and scales from there. These link through to how RMAI works.
What a defensible result looks like.
We are new to this sector: these are independent reference benchmarks, not our own results. They are published, third-party results in healthcare operators — illustrative of the target RMAI builds toward, with a clinician in the loop throughout. They are not RMAI client claims. The strongest independent evidence is enterprise-scale; SME-scale figures are vendor-reported and more modest.
Considering AI for your healthcare practice?
The two-week diagnostic is the right place to start. Fixed scope, fixed price. We’ll tell you whether the pattern fits and what the build would look like.