AI for aged care, grounded in your own care records and policies.
AI for aged care is grounded, auditable software that RMAI builds on your own assessments, care records, and policies — so care plans, shift handovers, and care-minute evidence are drafted, checked, and cited in minutes, with a clinician signing off every record.
What actually slows an aged-care provider down.
The margins are gone — most homes are running at a loss — and the rules just got harder, all while the workforce stays thin. But the binding constraint is not clinical skill; it is operational: a documentation, compliance-evidence, and handoff load that pulls scarce clinical staff off the floor. Each one is a documents-and-data problem, which is exactly where grounded AI pays back.
Carers lose much of the shift to paperwork
Legacy care systems demand redundant narrative entry across disconnected modules, so documentation is finished after hours — the unpaid or overtime "pyjama time" that should have been direct care. The skill is not the bottleneck; the keyboard is.
Care-minute targets are mandatory and tracked by hand
Residential homes must deliver 215 total plus 44 RN care minutes per resident per day and report coverage monthly through GPMS, yet many still track it in spreadsheets against short-notice leave. From April 2026 a metro home that falls short loses up to $33.41 per resident per day.
Vague clinical notes quietly underclaim your funding
AN-ACC assessors fund only what is documented. Time-pressured carers write "assisted with walking" instead of "two-person assist, 50m", so genuine care complexity goes unrecorded and an under-classified bed can leak around $30 a day in legitimate funding (illustrative).
Systems don't talk, so data is re-keyed and lost
Researchers found 94.6% of residential residents had medication-list discrepancies between facility and GP records. Intake, clinical, rostering and finance tools rarely share data, forcing duplicate entry and losing critical detail at every handover and transfer.
What changes once care work is grounded in your own records.
Providers working with RMAI recover clinical hours and tighten their audit trail at the same time. The tools work with your existing care-management and rostering systems — they read from them and do not create a second source of truth; a named approver can reject any draft, and every decision is logged and attributed. The outcomes below are illustrative of shipped patterns; every one keeps a clinician on the final call — nothing finalises a care record on its own.
The questions leaders ask first.
The questions below are the ones RMAI hears in the first call — on safety, staffing, compliance, cost, and feasibility.
What the time recovered is worth.
Move the sliders for your own volumes; the benchmark shows where shipped builds have landed.
| Task | Before | After |
|---|---|---|
| Care-plan first draft | ~20 min | 36 sec (review) |
| Care-minute / RN compliance tracking | manual spreadsheets | 75% less time |
| Shift handover summary | verbal + late notes | 1-page brief in minutes |
| Home-care visits delivered as planned | ~60% | ~90% |
What RMAI has built for this sector.
The applications below are grounded, human-in-the-loop tools for this sector — some already built and shipped, some scoped from real briefs. Ask us which is which.
SIRS Incident Triage Assistant

Reads each incident note against the eight reportable-incident categories, surfaces the likely category, priority and notification deadline, and drafts the notice for a clinician to approve — so a night-shift under-call doesn't quietly blow the 24-hour window.
Shift Handover Summariser

Turns a shift's scattered progress and incident notes into a one-page ISBAR-structured handover — vitals, meds, intake, mobility, falls, mood — with the source note quoted on every line and clinical risks flagged for the RN.
Care Policy Concierge

Answer staff "what does our policy say?" questions from your approved document library — with the clause cited, and a refusal when the answer isn't there.
Care Policy AskMe

Answers a carer's policy or procedure question at the point of care from your own approved library — quoting the section, naming the document and version, and saying so when the answer isn't there.
Plan Reassessment Drafter

Turns a participant's file into a first-draft plan reassessment report your coordinator edits down, instead of starting from a blank page.
Patient-Message Triage Copilot

Sorts the patient inbox before it reaches a clinician — classifies each portal or email message, scores urgency, routes it to the right queue, and drafts a holding reply for staff to approve, while escalating anything that reads clinically urgent instead of answering it.
Clinical Note Generator

Turn the consultation you just had into a structured SOAP note before the next patient walks in — drafted from the audio, reviewed and signed off by the clinician.
Complaint Response Agent

Triages every patient complaint the moment it lands, flags the clinical-safety ones, and drafts a policy-grounded acknowledgement for staff to approve.
Clinic Policy Concierge

Staff ask about an SOP, a payer rule, a consent requirement or a care protocol and get a short answer that quotes the exact section it came from — and says "not in your documents" instead of guessing.
Support-Coordination Report Drafter

Turns weeks of scattered case notes and provider service logs into a draft progress report mapped to the participant's plan goals, with the source note cited behind every claim — the coordinator reviews and signs.
NDIS Service Agreement Generator
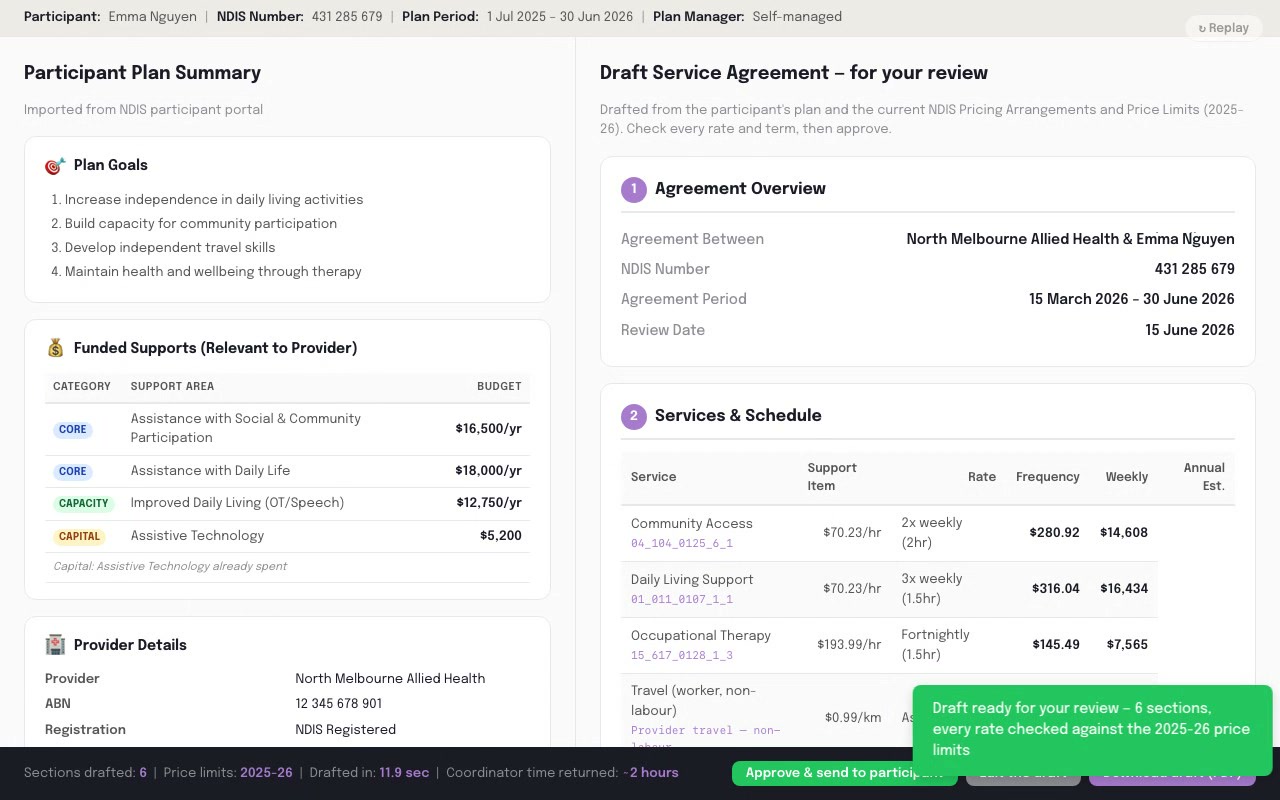
Draft a participant service agreement from the plan and the current price limits in minutes — every rate, support item and cancellation term in place before a coordinator signs off.
Reportable-Incident Signal Triage

Reads the daily progress-note flow, quotes the plain-language wording that looks like a possible reportable incident, rates its confidence, and routes it to your Approver against the 24-hour clock — flagging, never lodging.
NDIS Progress Note to Claim

Turn a support worker's session note into a draft NDIS claim — the right support item, the matching plan goals, and the compliance checks already done, for a person to approve.
Demand-Matched Roster Builder

A draft weekly roster matched to your forecast demand and held inside the labour budget, with every shift checked against the Restaurant Award and anything risky flagged for the manager to fix before sign-off.
Award Rate Checker

Reconciles every payslip line against the modern award before the pay run leaves, so an underpaid weekend penalty or missed allowance gets caught — and corrected — before it becomes a wage-theft exposure.
Prompts you can use today, for free.
Sector-specific prompts RMAI uses as starting points. Copy one and run it against de-identified samples — or inside an approved private environment — to see the shape of the answer before you talk to us.
How RMAI would work with you.
Every engagement starts with the diagnostic and scales from there. These link through to how RMAI works.
Independent industry results.
Independent industry results — not RMAI client claims. These are published third-party results from comparable Australian providers (ECH, MercyCare, Australian Unity), illustrative of the target RMAI builds toward, with a clinician in the loop throughout.
Considering AI for your aged-care operation?
The two-week diagnostic is the right place to start. Fixed scope, fixed price. We’ll tell you whether the pattern fits and what the build would look like.